Sequential conditioning may offer comparable remission and survival rates to intensive induction chemotherapy pre-allogeneic HCT for relapsed refractory AML patients
Dec 2022
This study is the first randomized controlled trial examining intensive induction chemotherapy compared to sequential conditioning before allogeneic hematopoietic cell transplantation (alloHCT) in relapsed/refractory acute myeloid leukemia (AML) patients.
Results presented at the 64th Annual Meeting and Exposition of the American Society of Hematology (ASH) showed no statistically significant difference in complete remission (CR) or overall survival (OS) between patients receiving intensive induction chemotherapy and those receiving thorough monitoring and sequential conditioning immediately before alloHCT.
Background
Patients with AML in CR before alloHCT have historically had superior outcomes to those not in CR. However, the benefit of inducing CR with an additional round of intensive chemotherapy before alloHCT for patients with relapsed/refractory AML is not fully known.
Earlier studies have demonstrated the successful use of sequential conditioning within 12 days of alloHCT with high-dose cytarabine or melphalan followed by reduced-intensity conditioning, which led to good results. Therefore, the study team questioned whether intensive induction chemotherapy before alloHCT improves outcomes compared to watchful waiting and sequential conditioning.
Study Details
The study cohort included 281 adult patients with relapsed/refractory AML with a poor response after first induction therapy (n=183) or AML relapse (n=98). Median patient age was 61 years old. Patients were eligible for intensive chemotherapy and alloHCT with either a matched sibling donor (MSD), a single-mismatched unrelated donor (9/10 MMUD), or an ongoing search with two potential unrelated donors with higher than 90% matching probability.
Patients were randomized into two arms, a remission induction strategy with high-dose chemotherapy and subsequent alloHCT (RIST-arm) or disease control before sequential conditioning and alloHCT (DISC-arm). Watchful waiting was recommended in the DISC-arm, but low-dose chemotherapy and single-dose mitoxantrone were permitted for disease control.
The primary endpoint was treatment success, defined as CR at day 56 after alloHCT. The goal was to show that treatment in the DISC-arm was not worse than in the RIST-arm by a 5% margin. Secondary endpoints were overall survival (OS) and leukemia-free survival (LFS) from CR at day 56.
Results
Most patients in the DISC-arm (76%) were monitored with watchful waiting before starting sequential conditioning, while some patients (24%) needed disease-control measures. All patients in the RIST-arm received high-dose chemotherapy induction, in which 46% of patients achieved CR. A few patients (5) received a second course of intensive chemotherapy, and the remaining patients proceeded to alloHCT without further attempts to induce a CR.
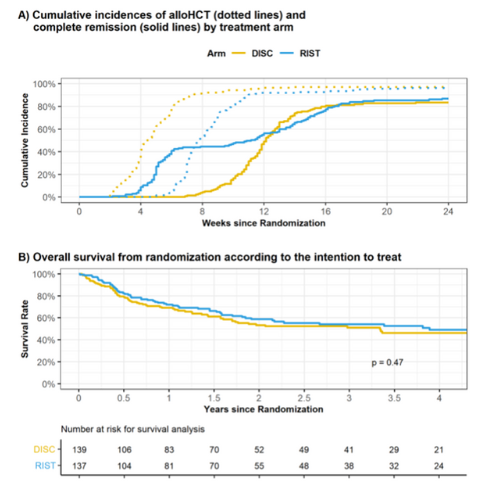
The median time to alloHCT was 4 weeks in the DISC-arm and 8 weeks in the RIST arm. At 24 weeks from randomization, 98% and 96% of patients had been transplanted in the DISC and RIST arm, respectively. Figure 1A shows alloHCT and CR achievement in both arms.
The primary endpoint was reached by 84% of patients in the DISC-arm and 81% of those in the RIST-arm. The 1-year LFS from CR at day 56 was approximately 72% in the DISC-arm and 70% in the RIST-arm, with a median follow-up of 37 months from randomization. The OS was comparable between both arms at 1- and 3-years post-transplant, as shown in Figure 1B.
Key Takeaways
This novel study provides the first randomized controlled trial addressing the perceived benefits of intensive induction chemotherapy before alloHCT for patients with relapsed/refractory AML.
Patients receiving high dose chemotherapy before alloHCT did not show a higher overall success rate and did not confer a survival advantage over those receiving treatment by watchful waiting before sequential conditioning and immediate alloHCT. The sequential conditioning approach resulted in comparable overall CR rates and survival. However, the use of the same induction strategy that was initially unsuccessful on the RIST-arm and the use of disease reducing chemotherapy on the DISC-arm do complicate the interpretation of the results.
These data may support the potential to proceed with sequential conditioning and alloHCT without prior remission induction chemotherapy if a donor is readily available. In addition, the median time to transplant for sequential conditioning was half the time of intensive induction chemotherapy, likely due to donor availability from early donor search. This data further supports the impact of early donor search at the time of AML diagnosis for optimal patient outcomes.
Figure 1
Stelljes M, et al., ASH Abstract